
Why Gut Healing is the Missing Variable in Celiac Recovery
By Jane Huang · Private Kitchen 44
Removing the trigger is not the same as rebuilding the system. Most celiac protocols stop at the first step. This article is about the second.

THE STANDARD SCRIPT — AND WHY IT’S INCOMPLETE
Here’s what most people with celiac disease are told:
“Remove gluten. Your gut will heal. You’ll be fine.”
And they follow it. Strictly. Sometimes religiously. And yet — brain fog persists. Fatigue doesn’t lift. Skin keeps flaring. Digestion is still chaotic. Lab markers don’t normalize. The body is still on fire even though the trigger has been removed.
Why?
Because removing the trigger is not the same as rebuilding the system.
If someone has been punching a wound for years and you stop the punching — the wound doesn’t automatically close overnight. The tissue is damaged. The architecture needs to be rebuilt. The immune memory needs to be recalibrated. The ecosystem needs to be re-established.
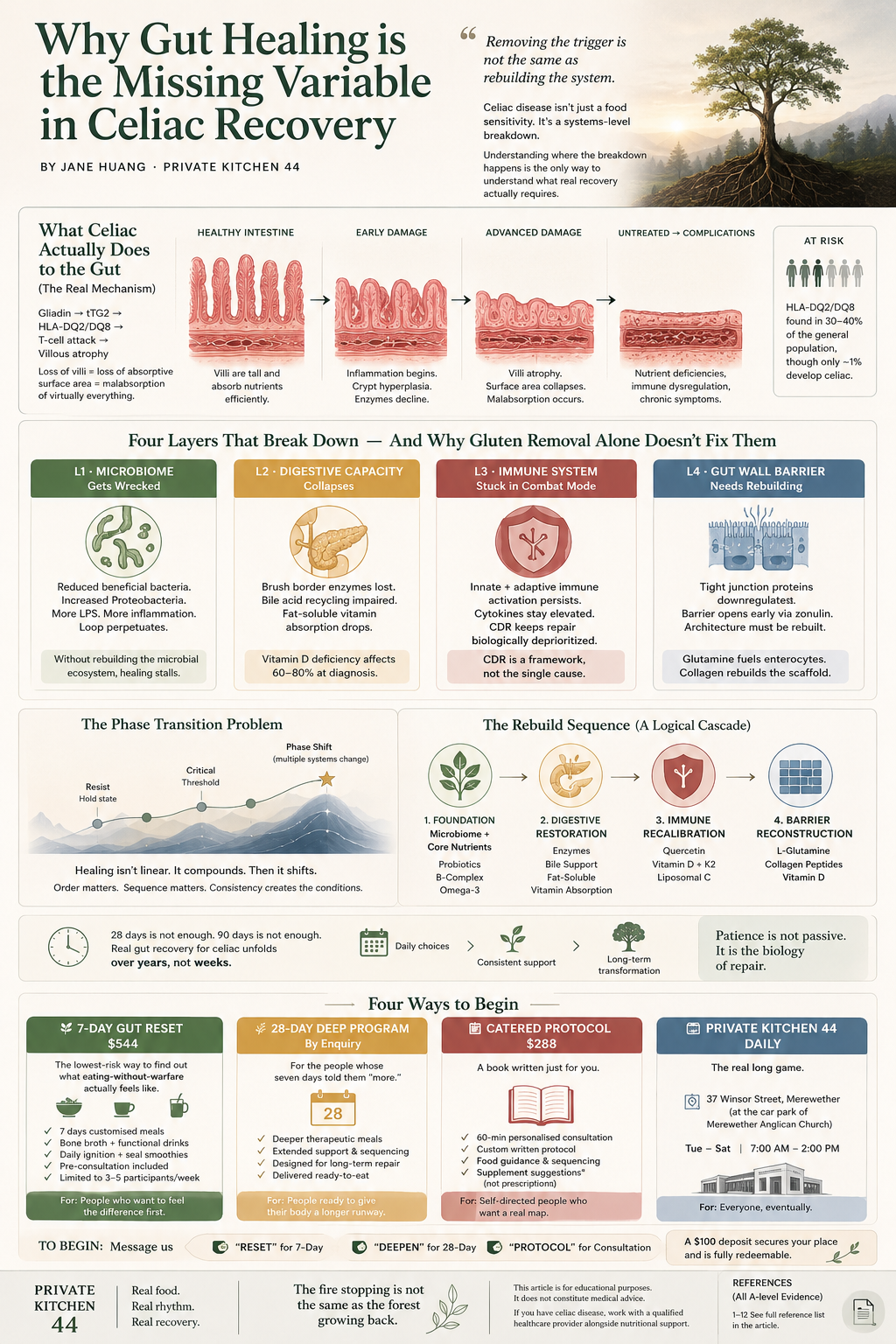
Celiac disease isn’t just a food sensitivity. It’s a systems-level breakdown — and understanding where the breakdown happens is the only way to understand what real recovery actually requires.

WHAT CELIAC ACTUALLY DOES TO THE GUT
Celiac disease is an autoimmune condition triggered by gluten — specifically gliadin peptides — in genetically susceptible individuals (HLA-DQ2/DQ8 positive, found in 30–40% of the general population, though only about 1% develop celiac).¹
When gliadin enters the small intestine, tissue transglutaminase (tTG2) modifies it. The modified gliadin is presented to T-cells by HLA-DQ2/DQ8 molecules. The immune system launches a CD4+ T-cell mediated attack — not just on the gliadin, but on the intestinal tissue itself.
The result: villous atrophy. The finger-like projections (villi) lining your small intestine — which exist to maximize absorptive surface area — get flattened. What should look like a lush carpet becomes a smooth, barren floor.
Loss of villi = loss of absorptive surface area = malabsorption of virtually everything: iron, calcium, magnesium, zinc, fat-soluble vitamins (A, D, E, K), B12, folate, and more.²
But villous atrophy is the headline. The full story is deeper.
FOUR LAYERS THAT BREAK DOWN — AND WHY GLUTEN REMOVAL ALONE DOESN’T FIX THEM

Layer 1 · The Microbiome Gets Wrecked
Long before diagnosis, and dramatically after years of active celiac, the gut microbiome shifts into a profoundly dysbiotic state.
Research shows celiac patients have significantly reduced Lactobacillus and Bifidobacterium species and elevated Proteobacteria — a pattern associated with intestinal inflammation and compromised barrier function. Even on a strict gluten-free diet, microbiome composition often remains abnormal for years.³
The mechanism chain:
Villous inflammation → altered gut motility and pH → selection pressure on bacterial populations → bloom of gram-negative bacteria → increased lipopolysaccharide (LPS) → more immune activation → more inflammation → slower mucosal healing.
It’s a loop. The microbiome damage perpetuates the inflammatory state that prevents the gut from healing.
Without actively rebuilding the microbial ecosystem, the gut is trying to heal itself in a hostile internal environment.
Layer 2 · Digestive Capacity Collapses
Brush border enzymes — the enzymes physically embedded in the tips of the villi — are among the first casualties of villous atrophy.
Lactase. Sucrase. Maltase. Gone, or severely depleted.
This is why so many newly diagnosed celiac patients are also temporarily (or persistently) lactose intolerant — not because dairy is a primary problem, but because the enzyme machinery that processes it has been physically destroyed.
Beyond sugar-splitting enzymes, bile acid recycling is also disrupted. The terminal ileum (damaged in celiac) is where bile acids are reabsorbed. Impaired bile acid recirculation → reduced bile availability → poor fat emulsification → fat malabsorption → deficiencies in fat-soluble vitamins D, A, E, K.
Vitamin D deficiency is highly prevalent in celiac at diagnosis — found in 60–80% of newly diagnosed patients across multiple cohorts.⁴ Vitamin D is not just a nutrient — it’s a critical immune modulator and a tight junction regulator. Its absence directly undermines the mucosal healing process.
Remove gluten. But if bile flow is sluggish and enzyme capacity is flat — nutrients from the best possible food still don’t get in.
Layer 3 · The Immune System is Stuck in Combat Mode
Celiac is defined by an adaptive immune response — T-cells, antibodies (anti-tTG IgA, anti-DGP), the whole machinery. But the innate immune system is also activated. Intraepithelial lymphocytes (IELs) are elevated. Mast cells are hyperactivated. Cytokines — IL-15, IL-21, IFN-γ, TNF-α — are chronically elevated.
Even after gluten is removed, immune memory persists. The body has been in a war state for years. The inflammatory signalling infrastructure doesn’t just switch off because the enemy is gone.
This is what’s called Cell Danger Response (CDR) — a concept articulated by Robert Naviaux at UC San Diego.⁵ When cells detect chronic threat, they lock into a defensive metabolic state. Mitochondrial function prioritizes ATP for defense, not repair. Tight junction protein synthesis drops. Mucosal regeneration slows.
The body isn’t failing to heal. It is physically, biochemically unable to prioritize repair while CDR is active.
CDR is not proposed here as the single cause of celiac pathology, but as a useful systems-level framework for understanding why repair can remain biologically deprioritized even after the primary trigger is removed.
Clinically: this is why some celiac patients experience persistent symptoms even on strict gluten-free diets with negative antibody panels. The tissue may be structurally healing. But the immune tone hasn’t reset. Histamine intolerance, mast cell hyperreactivity, food sensitivities expanding — these are often L3 never-turned-off signatures.
Layer 4 · The Gut Wall Barrier Needs to Be Physically Rebuilt
The intestinal barrier is not one thing. It’s an architecture:
· Mechanical layer — epithelial cells connected by tight junction proteins (Claudin family, Occludin, ZO-1)
· Mucus layer — secreted by goblet cells, houses commensal bacteria
· Immune barrier — secretory IgA, Paneth cells, intraepithelial lymphocytes
· Chemical barrier — bile acids, defensins, antimicrobial peptides
In active celiac, and in the extended aftermath, all four sub-layers are compromised.
Tight junction proteins are directly regulated by zonulin — a protein that gliadin triggers even in the early stages of exposure. Fasano and colleagues established that gliadin increases intestinal permeability via zonulin even before the immune cascade fully fires.⁶ This is why some sensitive celiac patients react to trace gluten long before antibody levels rise — the barrier opens first.
L-Glutamine is the primary fuel for intestinal epithelial cells (enterocytes). Not glucose — glutamine. Without adequate glutamine supply, enterocytes cannot synthesize tight junction proteins at the rate needed to rebuild the physical wall. This is one of the most consistently supported mechanisms in gut repair literature.⁷,⁸
Collagen peptides — providing glycine and proline — supply the amino acid substrate for the extracellular matrix that gives the epithelium its structural scaffold.
THE PHASE TRANSITION PROBLEM: WHY HEALING ISN’T LINEAR
The body is not a linear machine where input A predictably produces output B. It’s a complex adaptive system — and complex systems don’t change gradually. They hold state, resist, and then shift phase at critical thresholds.⁹
Water at 99°C is still water. One more degree — phase transition.
The gut ecosystem works the same way. You can be doing everything technically correct — strict gluten-free diet, taking supplements, resting — and feel like nothing is changing. Then at some threshold of ecosystem recovery, multiple systems shift simultaneously: energy comes back, inflammation drops, sleep deepens, skin clears. Not because one thing worked, but because the system crossed a critical point.
Consistency compounds. Phase transitions are not felt until they happen.
The order in which you rebuild matters enormously. You cannot skip the microbiome layer and go straight to immune suppression. You cannot patch the barrier without first reducing the inflammatory load that’s actively dismantling it. Systems have sequences.
A note on timescale. After eight years of clinical work: 28 days is not enough. 90 days is not enough. The numbers that appear in “reset” marketing are consumer-psychology thresholds, not biological timelines. Real gut recovery for someone with celiac disease unfolds over years, through the daily, unspectacular work of eating in a way that stops asking your body to fight.
THE REBUILD SEQUENCE
Foundation · microbiome + core nutrients
High-potency multi-strain probiotics are the biological scaffolding for every downstream function. A large proportion of the body’s serotonin is synthesised in the gut, short-chain fatty acids are generated there, and local immune regulation depends on a functioning microbial ecosystem. Methylated B-complex addresses the near-universal B12 and folate depletion. Omega-3 fatty acids (EPA/DHA) have been repeatedly associated with modulation of inflammatory signalling pathways.
Digestive restoration · L2
Comprehensive digestive enzymes support nutrient extraction while native brush border enzymes recover. Bile support restores fat-soluble vitamin absorption. This isn’t compensating for a permanent deficiency — it’s scaffolding a functional process while the architecture repairs.
Immune recalibration · L3
Quercetin directly stabilizes mast cells and inhibits histamine, leukotriene, and cytokine release — mechanistically relevant to the mast cell hyperreactivity pattern common in post-active celiac.¹⁰ Vitamin D is a direct transcriptional regulator of claudin family tight junction proteins via the Vitamin D Receptor (VDR), and modulates both innate and adaptive immune responses.¹¹,¹²
Physical barrier reconstruction · L4
L-Glutamine: commonly used in clinical gut repair protocols — primary fuel for the cells that are the wall. Collagen peptides provide glycine and proline for extracellular matrix reconstitution. Vitamin D directly upregulates tight junction protein gene expression via the VDR pathway.¹¹
WHAT THIS LOOKS LIKE IN PRACTICE
The person who has been gluten-free for two years and still has persistent fatigue, ongoing brain fog, expanding food sensitivities, lab markers that remain “borderline,” skin issues that won’t resolve — is almost certainly experiencing incomplete system recovery at one or more of these four layers.
The gut stopped being attacked. But it was never rebuilt.
This is not a mystery. It’s a sequence problem.
Removing the trigger is not the same as rebuilding the system. Both matter. Only one gets talked about.
WHERE PRIVATE KITCHEN 44 COMES IN
You cannot supplement your way out of celiac. You rebuild the daily conditions through food.
Not because supplements don’t matter — they do. But because the foundation underneath every supplement is the same question: what food is your gut actually meeting, every day, for the next several years?
This is what Private Kitchen 44 exists to do. Not deliver a “cure.” Not promise a transformation. Build a physical kitchen architecture, refined over eight years, where people whose guts have been at war for decades can finally eat food that doesn’t trigger the war.
That’s the entire offering. Simple. Boring. Slow. Consistent.
FOUR WAYS TO BEGIN
🌿 7-Day Gut Reset · $544
The lowest-risk way to find out what eating-without-warfare actually feels like.
Seven days of customised meals designed for your specific situation. Many people first notice the difference through digestion, heaviness, energy, or post-meal comfort. It’s not a treatment. It’s not a transformation. It’s your body’s first chance to taste what the literature describes.
What it includes:
· Pre-consultation questionnaire + system assessment
· 7 days of customised lunches (main + bone broth + functional drink)
· Daily ignition smoothie + evening seal smoothie
· Limited to 3–5 participants per week
For: People who want to feel the difference before committing to anything bigger.
Send: RESET
🌾 28-Day Deep Program
For the people whose seven days told them “more.”
If after the 7-Day Reset your body said yes, keep going — this is what comes next. A deeper program of P44 therapeutic meals, prepared in our kitchen and delivered into your hands, designed for the gut that has been at war for ten, twenty, thirty years.
Available by enquiry, after the 7-Day program.
For: People who have already tasted the difference and want their body to have a longer runway.
Send: DEEPEN
📋 Catered Protocol · $288
For the self-directed: a book written just for you.
One-hour personalised consultation + a fully written protocol designed around your specific gut situation, food tolerances, nervous system state, and life context. No coaching, no monthly fee. You take it home and do it your way, at your pace, in your kitchen.
What you get:
· 60-minute one-on-one consultation
· Custom written protocol (printed + digital)
· Specific food guidance, sequencing, and rationale
· Supplement suggestions (taken to your own practitioner)
For: People who want a real map rather than a hand to hold.
Send: PROTOCOL
🍱 Private Kitchen 44 · Daily
The real long game.
The most powerful thing for a celiac gut isn’t a reset package. It’s a kitchen you can come back to, again and again, and trust completely. Real recovery takes years — through the daily work of eating in a way that stops asking your body to fight.
That kitchen is here.
📍 37 Winsor Street, Merewether
(at the car park of Merewether Anglican Church)
⏰ Tuesday – Saturday · 7:00 AM – 2:00 PM
A $100 deposit secures your place in any pathway and is fully redeemable toward your meals.
REFERENCES
- Pinto-Sánchez MI et al. Beyond the HLA Genes in Gluten-Related Disorders. Frontiers in Nutrition. 2020;7:575844.
- Bledsoe AC et al. Micronutrient Deficiencies Are Common in Contemporary Celiac Disease. Mayo Clinic Proceedings. 2019;94(7):1253–1260.
- Cenit MC et al. Intestinal Microbiota and Celiac Disease: Cause, Consequence or Co-Evolution? Nutrients. 2015;7(8):6900–6923. PMID: 26287240
- Zanchi C et al. The Effect of a Gluten-Free Diet on Vitamin D Metabolism in Celiac Disease. Metabolites. 2023;13(1):74.
- Naviaux RK. Metabolic Features of the Cell Danger Response. Mitochondrion. 2014;16:7–17. PMID: 23981537
- Fasano A et al. Zonulin, a Newly Discovered Modulator of Intestinal Permeability, and Its Expression in Coeliac Disease. The Lancet. 2000;355(9214):1518–1519.
- van der Hulst RR et al. Glutamine and the Preservation of Gut Integrity. The Lancet. 1993;341(8857):1363–1365. PMID: 8098788
- Rao R, Samak G. Role of Glutamine in Protection of Intestinal Epithelial Tight Junctions. Journal of Epithelial Biology and Pharmacology. 2012;5:47–54. PMID: 25810794
- Scheffer M et al. Early-Warning Signals for Critical Transitions. Nature. 2009;461(7260):53–59.
- Weng Z et al. Quercetin Is More Effective than Cromolyn in Blocking Human Mast Cell Cytokine Release. PLOS ONE. 2012;7(3):e33805.
- Zhang YG et al. Tight Junction CLDN2 Gene is a Direct Target of the Vitamin D Receptor. Scientific Reports. 2015;5:10642.
- Chen S et al. Vitamin D Receptor Upregulates Tight Junction Protein Claudin-5. Mucosal Immunology. 2022;15(4):683–697.
© P44 · Private Kitchen 44 · Jane Huang 黄榛
Body in rhythm. Life in flow.
Merewether NSW · privatekitchen44.com
This article is for educational purposes only. It does not constitute medical advice. If you have celiac disease, work with a qualified healthcare provider alongside nutritional support.
